Comparison of caecal intubation rates between morning and afternoon colonoscopies at a tertiary hospital in Southwest Nigeria
Keywords:
Caecal intubation rates, morning, afternoon, Southwest NigeriaAbstract
Background: Caecal intubation is an important measure of the quality of colonoscopy. Information on the effect of the time of colonoscopy on caecal intubation rate (CIR) is scarce. This study aimed to compare the CIR between morning and afternoon colonoscopies at the University College Hospital, Ibadan, Nigeria.
Methods: A descriptive study of consenting patients referred for colonoscopy at the endoscopy unit of the University College Hospital, Ibadan, from January 2016 to March 2017. Bowel preparation consisted of liquid diet and Epsom salt. Pre-medications were intravenous Midazolam 2.5-5 mg and Pentazocine 1530 mg in titrated doses. Colonoscopy was performed using Olympus Exera III Videocolonoscope (CF HQ190L, Olympus UK). Morning procedures were those carried out between 8.30 am and 12.00 noon, while those after 12.00 noon were classified as afternoon procedures. Caecal intubation was considered successful when the medial wall of the caecum was visualized.
Results: Total of 177 colonoscopies were performed with 115 (65%) performed in the morning and 62
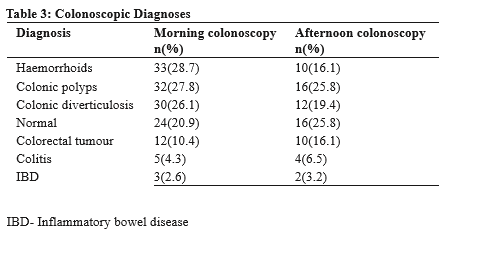
(35%) in the afternoon. In the morning, median age was 60 yrs, while in the afternoon, it was 61 yrs. Males (60.9% vs 58.1%) predominated in the morning, whereas females predominated in the afternoon (41.9% vs 39.1%), (p=0.72). In the morning, 100 (87%) patients had good/satisfactory bowel preparation, but 52 (83.9%) patients in the afternoon.(p=0.57). CIR was higher in the morning (90.4%), compared to afternoon (88.7%) (p=0.72).
Conclusion: There was no statistically significant difference between CIR in the morning and afternoon procedures.
References
Ball JE, Osbourne J, Jowett S, Pellen M, Welfare MR. Quality improvement programme to achieve acceptable colonoscopy completion rates: prospective before and after study. BMJ 2004;329:665-7
Marshall JB, Barthel JS. The frequency of total colonoscopy and ileal intubation in the 1990s. Gastrointest Endosc 1993;39:518-20
Rex DK, Bond JH, Winawer S, Levin TR, Burt RW, Johnson DA, et al. Quality in the technical performance of colonoscopy and the continuous quality improvement process for colonoscopy: recommendations of the U.S. Multi-Society Task Force on colorectal cancer. Am J Gastroenterol 2002;97:1296-1308
Wexner SD, Garbus JE, Singh JJ. A prospective analysis of 13,580 colonoscopies; reevaluation of credentialing guidelines. Surg Endosc 2001;15:251-61
Dafnis G, Granath F, Pahlman L, Ekbom A, Blomqvist P. Patient factors influencing the completion rate in colonoscopies. Dig Liv Dis 2005;37:113-8
Waye JD, Bashkoff E. Total colonoscopy: is it always possible? Gastrointest Endosc
;37:152-4
Saunders BP, Fukumoto M, Halligan S, Jobling C, Moussa ME, Bartram CI, et al. Why is colonoscopy more difficult in women?
Gastrointest Endosc 1996;43:124-6 8. Church JM. Complete colonoscopy: how often?
And if not, why? Am J Gastroenterol 1994;89(4):556-60
Bernstein C, Thorn M, Monsees K, Spell R, O'Connor JB. A prospective study of factors that determine cecal intubation time at colonoscopy. Gastrointest Endosc 2005;61:72-5
Cirocco WC, Rusin LC. Factors that predict incomplete colonoscopy. Dis Col Rect 1995;38:964-8
Chak A, Cooper GS, Blades EW, Canto M, Sivak MV. Prospective assessment of colonoscopic intubation skills in trainees. Gastrointest Endosc 1996;44:54-7
Harewood GC. Relationship of colonoscopy completion rates and endoscopist features. Dig Dis Sci 2005;50:47-51
Anderson JC, Gonzalez JD, Messina CR, Pollack BJ. Factors that predict colonoscopy: thinner is not always better. Am J Gastroenterol 2000;95:2784-7
Kim WH, Cho YJ, Park JY, Min PK, Kand JK, Park IS. Factors affecting insertion time and patient discomfort during colonoscopy. Gastrointest Endosc 2000;52:600-5
Sanaka MR, Shah N, Mullen KD, Ferguson DR, Thomas C, McCullough AJ. Afternoon colonoscopies have higher failure rates than morning colonoscopies. Am J Gastroenterol 2006;101:2726-2730
Wells CD, Heigh RI, Sharma VK, Crowell MD, Gurudu SR, Leighton JA, et al. Comparison of morning versus afternoon cecal intubation rates.
B M C G a s t r o e n t e r o l 2 0 0 7 ; 7 : 1 9
doi:10.1186/1471-230X-7-19
Singh S, Dhawan M, Chowdhry M, Babich M, Aoun E. Differences between morning and afternoon colonoscopies for adenoma detection in female and male patients. Annals of Gastroenterology 2016;29(4):497-501
Rex DK, Petrini JL, Baron TH, Chak A, Cohen J, Deal SE, et al. ASGE/ACG Taskforce on Quality in Endoscopy. Quality indicators for colonoscopy. Am J Gastroenterol 2006;101:873-
Yoon JH, Park DI, Shin JE, Kim SE, Jung SA, Lee SH, et al. Comparison of bowel preparation depending on completion time of polyethylene glycol ingestion and start time of colonoscopy. Intest Res 2010;8:24-29
Seo EH, Kim TO, Park MJ, Joo HR, Heo NY,
Park J, et al. Optimal preparation to colonoscopy interval in split-dose PEG bowel preparation determines satisfactory bowel preparation quality: an observational prospective study. Gastrointest Endosc 2012;75:583-590
Eun CS, Han DS, Hyun YS, Bae JH, Park HS, Kim TY, et al. The timing of bowel preparation is more important than the timing of colonoscopy in determining the quality of bowel cleansing. Dig Dis Sci 2011;56:539-544
Church JM. Effectiveness of polyethylene glycol antegrade gut lavage bowel preparation for colonoscopy: timing is the key! Dis Colon Rectum 1998;41:1223-1225
Kim TK, Kim HW, Kim SJ, Ha JK, Jang HH, Hong YM, et al. Importance of the Time Interval between Bowel Preparation and Colonoscopy in Determining the Quality of Bowel Preparation for Full-Dose Polyethylene Glycol Preparation. Gut and Liver 2014;8(6):625-631
Streett SE. Endoscopic colorectal cancer screening in women: can we do better? Gastrointest Endosc 2007;65:1047-1049
Akere A, Akande KO. Cecal intubation rate during colonoscopy at a tertiary hospital in South-west Nigeria: How frequent and what affects completion rate? Niger J Clin Pract 2017;20:303-6
Sadahiro S, Ohmura T, Yamada Y, Saito T, Taki Y. Analysis of length and surface area of each segment of the large intestine according to age, sex and physique. Surg Radiol Anat
;14:251-257
Waye JD. Completing colonoscopy. Am J Gastroenterol 2000;95:2681-2682 28. Rowland RS, Bell GD, Dogramadzi S, et al. Colonoscopy aided by magnetic 3D imaging: is the technique sufficiently sensitive to detect differences between men and women? Med Biol
Eng Comput 1999;37:673-679
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2023 Research Journal of Health Sciences

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Research Journal of Health Sciences journal is a peer reviewed, Open Access journal. The Journal subscribed to terms and conditions of Open Access publication. Articles are distributed under the terms of Creative Commons License (CC BY-NC-ND 4.0). (http://creativecommons.org/licences/by-nc-nd/4.0). All articles are made freely accessible for everyone to read, download, copy and distribute as long as appropriate credit is given and the new creations are licensed under the identical terms.